
![]() Secure delivery
Secure delivery ![]() UK clinicians
UK clinicians
Here’s what's included in the price:
Consultation
Answer a few questions about your health so we can get to know you better.
Free 24h delivery
Your treatment delivered in secure packaging, the very next day.
Aftercare
We’ll check in with you regularly to see how your treatment is going.

Here’s what's included in the price:
Consultation
Answer a few questions about your health so we can get to know you better.
Free 24h delivery
Your treatment delivered in secure packaging, the very next day.
Aftercare
We’ll check in with you regularly to see how your treatment is going.
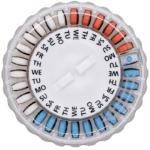
HRT Patches
What are HRT patches?
HRT patches are an easy-to-use and effective treatment for the symptoms of menopause. You stick one on your skin, usually below the waist, and it supplies you with hormones. These hormones can help to treat the frustrating symptoms of menopause and support your long-term health. And they come in either combined or oestrogen-only options, so they can be tailored to your specific needs.
You’ll use two different patches each week - one will be on for four days and the other for three. This helps to make sure that you’re getting the right amount of treatment from your patches. So although you’ll have to remember to change your patch on these days, you might find it easier or more convenient than taking something like a tablet (for example) on a daily basis.
How do HRT patches work?
HRT patches work by delivering hormones transdermally, meaning when applied, the hormones are absorbed through your skin.
Your oestrogen levels naturally decrease during menopause, leading to symptoms such as night sweats, hot flushes, mood changes and vaginal dryness. By delivering a steady flow of oestrogen into your system, oestrogen patches increase your oestrogen levels, helping manage your symptoms and reduce your risk of long-term problems like osteoporosis.
What are the benefits of using HRT patches?
HRT patches can be a good option for you for a number of reasons but, ultimately, it all comes down to preference.
So if you’re someone who’s not great at remembering to take daily tablets, patches can offer you at least a few days respite between having to remember your medication. They can be discreet too, and you don’t need to take them off or change them when you take a bath or shower.
Another positive of HRT patches is that they don’t come with the risk of getting certain side effects that come with tablets, such as heartburn or indigestion. And, also unlike tablets, they don’t increase your risk of blood clots.
They also deliver hormones to your whole body, which gives them the edge over vaginal oestrogen, which only treats localised symptoms such as vaginal dryness.
How long do HRT patches take to work?
It usually takes a few weeks for you to start feeling the benefits of any form of HRT, and patches are no different. But this isn’t the same for everyone – you may notice that you start to feel better in a shorter time-frame.
If you’re still not feeling the benefits after a month or two, it may be that you need to increase your dose, or switch to a different HRT.

This page was medically reviewed by Dr Daniel Atkinson, GP Clinical Lead on May 27, 2026. Next review due on May 27, 2029.
How we source info.
When we present you with stats, data, opinion or a consensus, we’ll tell you where this came from. And we’ll only present data as clinically reliable if it’s come from a reputable source, such as a state or government-funded health body, a peer-reviewed medical journal, or a recognised analytics or data body. Read more in our editorial policy.
HRT Patches
Oestrogen-only or combined: what’s the difference?
The form of HRT you take (oestrogen-only or combined) will depend on whether you’ve had a hysterectomy or not. This is because when you take oestrogen-only HRT without progestogen it can increase your risk of womb cancer. Taking a progestogen alongside it works to protect you from this risk.
This doesn’t mean you have to take them both in one treatment if you don’t want to. It just means that if you take oestrogen-only HRT you’ll have to take a separate progesterone in whichever form you like.
Continuous versus sequential
Continuous HRT delivers a steady dose of hormones into your system at a consistent level, whereas sequential HRT delivers variable doses, designed to either mimic your menstrual cycle or induce a three-monthly bleed. But which version is best for you?
Well this is where it gets a little more complicated.
Whether you take continuous or sequential HRT depends on which stage of the menopause you’re in. Generally speaking, sequential HRT is for women who are still getting periods (i.e. those in the perimenopausal stage), whereas continuous is for those in the postmenopausal stage (who are no longer getting periods).
There are two kinds of sequential HRT: monthly cyclical and three-monthly cyclical. The one you take will be down to your preference, as well as your clinician’s recommendation. Monthly cyclical tends to induce a monthly bleed, whereas three-monthly cyclical will induce a bleed every three months.
Can you switch from one form of HRT to another?
You can switch from one form of HRT to another, yes (once you get the ‘go-ahead’ from your clinician). You’ll just need to make sure that you’re still taking the right form of HRT for the stage of menopause that you’re at. So whether you want to change from HRT patches to gel, gel to patch, tablet to patch or gel to patch, it’s not a problem. It’s all about making sure you’re still getting the right level of hormones for your health.
And if you’ve been taking sequential HRT for a few years this can usually be changed to continuous HRT. This should lead to your periods stopping, but you may still get some unpredictable bleeding if you’re not postmenopausal.
This page was medically reviewed by Dr Daniel Atkinson, GP Clinical Lead on May 27, 2026. Next review due on May 27, 2029.
How we source info.
When we present you with stats, data, opinion or a consensus, we’ll tell you where this came from. And we’ll only present data as clinically reliable if it’s come from a reputable source, such as a state or government-funded health body, a peer-reviewed medical journal, or a recognised analytics or data body. Read more in our editorial policy.
HRT Patches
This page was medically reviewed by Dr Daniel Atkinson, GP Clinical Lead on May 27, 2026. Next review due on May 27, 2029.
How we source info.
When we present you with stats, data, opinion or a consensus, we’ll tell you where this came from. And we’ll only present data as clinically reliable if it’s come from a reputable source, such as a state or government-funded health body, a peer-reviewed medical journal, or a recognised analytics or data body. Read more in our editorial policy.

Medroxyprogesterone
MedroxyprogesteroneProgestogen-only tablet that helps lower oestrogen-related side effects. Generic version of Provera.
- Starting from £32.95

Conjugated Oestrogens/Medroxyprogesterone
Conjugated oestrogens + MedroxyprogesteroneCombined HRT treatment for menopause relief. Similar to Indivina and Premique.
- Starting from £79.95

Nalvee
DydrogesteroneA synthetic progestogen tablet that balances your oestrogen during HRT.
- Starting from £39.95

Utrogestan and Oestrogel Pack
Micronised progesterone / EstradiolHRT that comes together in a pack. Contains an oestrogen gel and progesterone capsule.
- Starting from £77.95
Estradot
EstradiolSimple treatment for menopause symptoms. Estradot is a HRT patch you change just twice a week.
- Starting from £39.95

Oestrogel
EstradiolHRT gel you rub into your skin. It has an easy-to-use pump pack for menopause relief.
- Starting from £44.95
Evorel Sequi
Estradiol/NorethisteroneSequential dose patch. Use to manage menopause symptoms if you still have periods.
- Starting from £47.95

Sandrena
EstradiolOestrogen-only gel that's stronger than oestrogel. Used alongside a progestin for combined HRT.
- Starting from £44.95
Evorel Conti
Estradiol/NorethisteroneCombined continuous HRT patch. Used it's been more than 12 months since your last period.
- Starting from £47.95

Kliovance
Estradiol/NorethisteroneLike Kliofem, but half the dose. HRT pill that’s good if you're sensitive to hormones.
- Starting from £47.95

Elleste Duet
Estradiol/NorethisteroneCombined sequential HRT tablets. For treating menopause symptoms if you still have periods.
- Starting from £39.95
Kliofem
Estradiol/NorethisteroneLike Elleste Duet, but continuous. Good for menopause symptoms if you no longer have periods.
- Starting from £47.95
Tibolone
TiboloneGeneric version of Livial. Hormone-free HRT that can improve mood and libido.
- Starting from £33.95

Utrogestan
Micronised progesteroneThe natural progesterone treatment. Taken alongside oestrogen to relieve symptoms of menopause.
- Starting from £37.95
Livial
TiboloneA daily tablet for post-menopausal symptoms. It’s hormone-free, but works just like female hormones.
- Starting from £41.95

Elleste Duet Conti
estradiol hemihydrate, norethisterone acetateLike Elleste Duet, but continuous. Which makes it best suited to postmenopausal women.
- Starting from £54.95
Lenzetto
EstradiolDaily form of HRT. Just spray it onto your skin to ease menopause symptoms.
- Starting from £37.95

Elleste Solo
EstradiolOestrogen-only HRT patches and pills. For if you've had a hysterectomy, or used with progestins.
- Starting from £39.95

Femoston
Estradiol/DydrogesteroneComes as a continuous or sequential tablet, depending on whether you're still having periods.
- Starting from £51.95
Estraderm MX
EstradiolOestrogen-only HRT patch. Change twice a week and reduce menopause symptoms up to 75%.
- Starting from £39.95

Zumenon
EstradiolOestrogen-only pill for menopause treatment. Same hormones as Elleste Solo, different brand.
- Starting from £37.95

Indivina
Estradiol/MedroxyprogesteroneContinuous combined HRT pill. Made for menopause symptoms if you haven't had a period in 1 year.
- Starting from £57.95
Progynova
EstradiolOestrogen only tablet or patch for women who've had a hysterectomy, or used alongside a progestogen in combined HRT.
- Starting from £37.95

Novofem
Estradiol/NorethisteroneLike Elleste Duet with fewer hormones. Effective HRT that’s good if you're sensitive to oestrogen.
- Starting from £41.95

Trisequens
Estradiol/NorethisteroneCombined treatment for menopause relief. Sequential pills for women who no longer have periods.
- Starting from £43.95
FemSeven
EstradiolA weekly oestrogen patch to combat symptoms of the menopause.
- Starting from £37.95
Out of stock 
Conjugated Oestrogens
Conjugated oestrogensDaily hormonal tablet to relieve menopause symptoms and reduce risk of osteoporosis.
- Starting from £74.95
Out of stock

FemSeven Conti
Estradiol/LevonorgestrelCombined HRT skin patch used by women who've had a year or more since their last period.
- Starting from £47.95
Out of stock
Premarin
Conjugated oestrogensOestrogen-only tablet that relieved menopausal symptoms. Often prescribed for women who’d had a hysterectomy.
- Starting from £69.95
Out of stock

Premique
Estradiol/MedroxyprogesteroneCombined continuous HRT pills, at a lower dose. Good if you're sensitive to hormones.
- Starting from £79.95
Out of stock
Tridestra
Estradiol/MedroxyprogesteroneExtended cycle tablet that's used in combined HRT.
- Starting from £61.95
Out of stock
Provera
Medroxyprogesterone acetateOestrogen only tablet or patch for women who've had a hysterectomy, or used alongside a progesterone in combined HRT.
- Starting from £32.95
Out of stock
Testogel
TestosteroneTestosterone gel you can rub onto your skin. Helps with loss of libido.
- Starting from £89.95
Dr Daniel Atkinson
Registered with GMC (No. 4624794)
Meet DanielMs Sanjeda Chowdhury

Registered with GPhC (No. 2202465)
Meet SanjedaMr Craig Marsh

Registered with GPhC (No. 2070724)
Meet Craig
Some treatments can cause side effects
Always read the leaflet that comes with your medication and tell us about any side effects you get.
Choose how you do healthcare.
We know health, but you know you.
Our experts tell you what’s safe, but you decide what’s best.

Consult on your own time
Answer a few questions and tell us about yourself. Get tailored advice from our clinicians so you can choose better.
Treatments to fit your life
Choose your treatment and how often you have it delivered.
Your health,
continued
We know things change. It’s the nature of life. We’ll check in regularly to make sure your treatment is still right for you.

Control at your fingertips
Pause. Change. Skip. Start again. Any time you like.
More general health
Here are some other things we can help with.

Acne
With a range of creams and tablets, we'll help you find the acne treatment that's right for you.

Allergies
Tablets, nasal sprays and eye drops. Get effective treatments to help you live your life, no matter your allergy.




Fungal nail
Choose from our range of tablets and solutions. Get ongoing care and support from our experts.

PrEP
Tablets you can take in different ways to help to lower your risk of HIV. Get advice and suggestions from our experts.

Stop smoking
Stop smoking treatments that can help you kick the habit forever, and reduce your risk of disease.

Weight loss
Tablets or injections. Tailored weight loss treatments combined with ongoing support from our experts.
Find treatment



